
Denied Due to Documentation: What Providers Need to Chart Better
Stop Losing Revenue to Documentation Denials
Why Documentation Is the Root Cause of Most Denials
What Is Clinical Documentation Improvement (CDI)?
A CDI program typically involves:
- Reviewing medical records for missing, inconsistent, or unclear information
- Querying providers to clarify diagnoses, procedures, or clinical indicators
- Collaborating with coders to validate that the selected ICD-10 and CPT codes reflect what was documented
- Tracking denial patterns and feeding that data back into documentation education
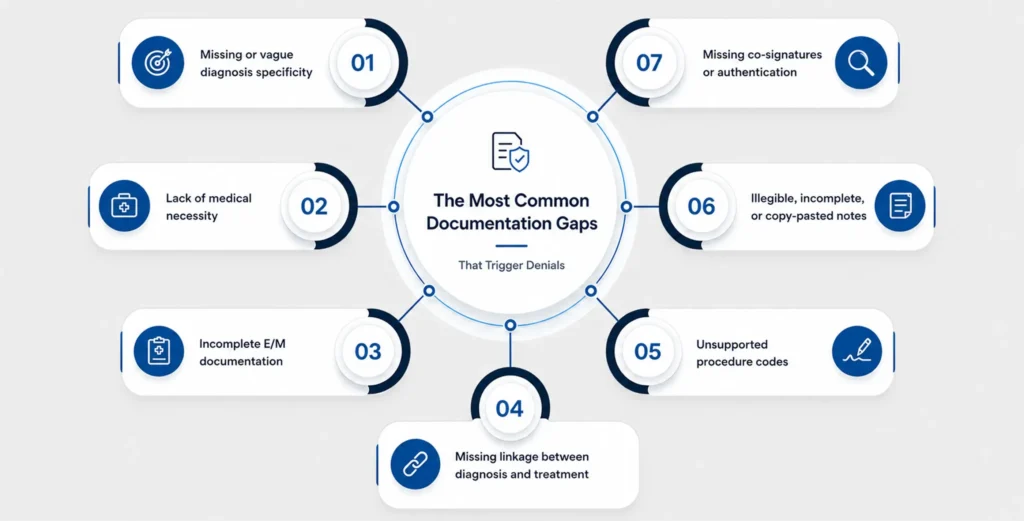
The Most Common Documentation Gaps That Trigger Denials
-
Missing or vague diagnosis specificity:
Documenting "diabetes" without specifying type, whether it is controlled or uncontrolled, and any complications gives payers very little to work with, and coders even less. -
Lack of medical necessity:
If the chart does not clearly explain why a service was medically necessary for this patient at this time, payers will question it. -
Incomplete E/M documentation:
With the updated CPT E/M guidelines, the level of service billed must be supported by documented medical decision-making or total time, and vague or copied notes will not hold up. -
Missing linkage between diagnosis and treatment:
Providers sometimes document a condition and a treatment separately without explicitly connecting them, leaving coders and payers to guess. -
Unsupported procedure codes:
When CPT codes are submitted without detailed procedure notes that justify the complexity, denials for upcoding or unbundling become likely. -
Illegible, incomplete, or copy-pasted notes:
Copy-forward notes that are not updated per visit are a major audit red flag and contribute significantly to denials. -
Missing co-signatures or authentication:
Notes that are not signed, dated, or authenticated by the treating provider may be rejected entirely.
Documentation vs. Denial: A Side-by-Side Look
| Documentation Issue | Likely Denial Type | Payer Justification |
|---|---|---|
|
Diagnosis listed without specificity |
Coding accuracy denial |
Cannot assign an appropriate ICD-10 code |
|
No documentation of medical necessity |
Medical necessity denial |
Service appears not clinically indicated |
|
E/M level not supported by the chart |
Downcoding or denial |
Billed level exceeds documented complexity |
|
Procedure note missing clinical detail |
Technical denial |
Insufficient information to process the claim |
|
Copy-pasted notes with no updates |
Audit-triggered denial |
Documentation does not reflect the actual visit |
|
Missing physician signature |
Administrative denial |
Record not authenticated |
|
Comorbidities not documented |
DRG downgrade (inpatient) |
Severity of illness understated |
What Payers Actually Want to See in the Chart
-
Clinical Indicators:
The record should clearly reflect the patient's presenting symptoms, history, examination findings, and any test results that support the diagnosis. -
Medical Decision-Making (MDM):
For E/M visits, especially, the chart needs to demonstrate the complexity of decisions made, the number and nature of problems, the data reviewed, and the risk of complications. -
Diagnosis Specificity:
Payers want ICD-10 codes that reflect the full picture, type, severity, laterality, acuity, and any comorbidities that affect care complexity. -
Treatment Justification:
There should be a clear, documented rationale connecting the diagnosis to the ordered tests, referrals, medications, or procedures. -
Continuity and Authenticity:
Notes should reflect what actually happened in that specific encounter, not a carry-forward from a prior visit. Each entry should be dated, timed, and signed.
How CDI Programs Reduce Denials and Protect Revenue
- Health systems with structured CDI programs experience a 25–30% reduction in claim denials, according to the Healthcare Financial Management Association (HFMA).
- In 2025, hospitals with active CDI programs reported an average revenue increase of $1.5 million and a 25% decrease in claim rejections.
- CDI reduces audit exposure by ensuring that comorbidities are clinically validated, procedures are categorized with full detail, and diagnoses meet payer coverage requirements.

Practical Tips for Providers to Chart Better Starting Today
For Providers:
- Be specific with every diagnosis. Instead of “hypertension,” document “essential hypertension, controlled, on an ACE inhibitor.” The more precise the diagnosis, the cleaner the code.
- Document the why. Always explain why a test was ordered, why a medication was prescribed, or why a referral was made. One extra sentence of clinical rationale can prevent a denial.
- Avoid copy-forward abuse. Review and update notes each visit. A chart that reads identically across six encounters is a denial (and audit) waiting to happen.
- Link conditions to treatment. Explicitly connect diagnoses to the services rendered in the same note.
- Document comorbidities that affect care. If a patient’s diabetes complicates a wound care visit, say so. These documented links support medical necessity and appropriate reimbursement.
For Billing Teams:
- Track denial patterns by reason code. If documentation-related denials are clustering around specific providers or service lines, that is where education should be focused.
- Flag pre-submission risk. Review high-value or complex claims before they go out, checking for documentation that may not support the codes selected.
- Create a query workflow. When documentation is unclear, there should be a fast, compliant process for the billing team to query the provider before the claim is submitted.
- Use denial data to drive training. Every denial is a data point. Use them to build targeted education for providers on what payers are pushing back on most.
How MaxRemind Supports Better Documentation and Cleaner Claims
At MaxRemind, we understand that revenue cycle performance starts long before a claim reaches a payer. Our team works alongside providers and billing staff to identify documentation gaps, reduce denials at their root cause, and protect the revenue your practice has already earned.
Denied Due to Documentation? Fix the Chart Before the Claim Fails
- What is the most common documentation issue that leads to claim denials?
-
One of the most common causes of documentation-related denials is a lack of diagnosis specificity. Incomplete descriptions of a patient's condition, missing clinical details, or failure to establish medical necessity can prevent payers from validating the services billed.
- How does Clinical Documentation Improvement (CDI) help reduce denials?
-
CDI programs help ensure medical records are accurate, complete, and compliant with payer requirements. By identifying documentation gaps before claims are submitted, CDI reduces denial rates, improves coding accuracy, and supports faster reimbursement.
- What do payers look for when reviewing medical documentation?
-
Payers typically look for clear clinical indicators, diagnosis specificity, documented medical necessity, treatment justification, and evidence that the services billed are supported by the provider's notes. Records should also be signed, dated, and specific to the encounter.
- Can poor documentation affect reimbursement even if coding is correct?
-
Yes. Even when the correct ICD-10 and CPT codes are selected, a claim can still be denied if the documentation does not support the diagnosis, procedure, or level of service billed. Documentation serves as the evidence behind every claim.
- How can providers improve documentation quality and prevent denials?
-
Providers can reduce denials by documenting diagnoses with greater specificity, clearly explaining medical necessity, linking treatments to conditions, updating notes for every encounter, and ensuring all records are complete, authenticated, and compliant with payer guidelines.
Transform Your
Practice with
AI-Powered EHR
Reduce administrative burden, streamline workflows, accelerate revenue, and deliver exceptional patient care.
- AI-Assisted Documentation
- HIPAA-Compliant Platform
- Faster Claims & Billing
- Specialty-Based Solutions
